Colonoscopy
..Tremendous progress in the field of fiberoptics has made it relatively simple for your doctor to examine the entire large intestine, or colon, with a procedure called colonoscopy. More accurate than a barium enema x-ray and much simpler than exploratory surgery, colonoscopy is a safe and highly effective diagnostic technique. After careful assessment, your doctor has decided that a colonoscopy is necessary to better evaluate and treat your condition. Since your cooperation is essential for a successful examination, it is important that you understand exactly what is to be done and why. If you have any additional questions or concerns after reading this information, please ask your doctor.
..What Is Colonoscopy?Colonoscopy is a medical term that has two parts - colono which refers to the colon, or large intestine, and scopy which means "looking into." Therefore,
colonoscopy is a test that enables your doctor to look inside your colon.
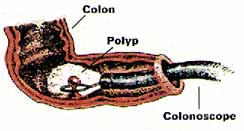
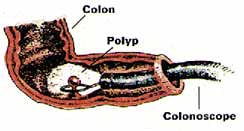
The instrument used to perform this test is the colonoscope: a long, flexible tube about the width of your index finger. Within the end of this tube is a miniaturized color-TV camera with a wide-angle lens. After passing this "scope" through the rectum and into your colon, your doctor then directly examines the lining of your lower digestive tract on a television monitor. In this manner, it is possible to evaluate intestinal inflammation, ulceration, bleeding, diverticulitis, colitis, colon polyps, tumors, etc. As part of your assessment, you may have undergone a barium enema examination of the colon, or "lower GI series." This technique, which utilizes x-rays, is helpful in identifying any areas of possible abnormality. X-rays are only shadows, however, and often do not fully demonstrate what is wrong. For example, the barium enema x-ray may miss nearly forty percent of colon polyps.
In the past, you also may have undergone a proctoscopic examination of the lower colon and rectum. Performed with a short, rigid, hollow tube, this limited procedure enabled the doctor to examine only the last ten inches of the large intestine. In most offices, the proctoscope has now been replaced by the flexible sigmoidoscope. This newer device enables your doctor to examine the last two feet of the colon while its flexibility affords the patient much greater comfort than does the rigid type of scope. The colonoscope offers a still greater advantage. With this longer flexible instrument, your doctor is usually able to directly examine the entire length of your colon - all five feet of its numerous twists and turns. In this manner, your doctor can be most certain about the condition of your colon.
..How You Can HelpYour cooperation is essential for a successful examination. There are certain things you can do to help before the test begins:
- Preparation A colonoscopy exam requires a thorough cleansing of the large intestine so that nothing impedes your doctor's view. The colon must be completely free of all solid waste. Since particles of stool can interfere with the examination, you will require a special dietary and laxative preparation on the day prior to the test. To be sure that you fully understand all aspects of the preparation, the GI Assistant or a member of the Nursing staff will review the preparation with you. It is critical that you follow the instructions as given. If the colon is not clean, the test - as well as the preparation - may have to be rescheduled. A few hints: It is best not to be constipated before the laxative preparation. This may lead to a temporary backup of the laxative solution, cramps, bloating, nausea, and vomiting. If you tend to be constipated, take one or two ounces of Milk of Magnesia the day before the laxative prep to "open up your pipes." This will make the actual preparation easier. If you develop mild distress during your prep, simply stop it for an hour or two and then resume it where you left off. If you develop severe abdominal cramps or persistent nausea and vomiting, stop the prep and call our office to reach our doctor on call. Of course, the laxative preparation will cause you to have many bowel movements. This may cause some rectal irritation and a small amount of bleeding. Many patients find that using Charmin Plus toilet tissue minimizes such rectal irritation. A nonprescription 1% hydrocortisone cream may also be soothing when applied to the rectal area after each bowel movement. Please avoid foods with many small seeds for a few days before the exam. They tend to linger in the colon and can clog our instruments. In addition, you must avoid all red-colored Jello products during your preparation as their red dye masks the lining of the colon.
- Medications Medications containing iron or Metamucil-like fiber can impair your doctor's view of the colon. If possible, they should be temporarily discontinued several days before the test. If you are taking chronic aspirin or Persantine therapy, diabetic medication, or the blood-thinner Coumadin, you will require special preparation and adjustment of your medicines before the test. Please call our office for instructions. All other routine medications may continue to be taken with a small sip of water, even on the day of the exam.
- What To Wear You will have to change into a patient gown before the examination. If this test is being done on an outpatient basis, you should wear, loose, comfortable, casual clothing that is easily removed and folded. Avoid girdles, pantyhose, or tight-fitting garments. Please leave your jewlery, valuables, and high heels at home. Transportation To minimize any discomfort, you will receive an injection before the colonoscopy. As this medication will make you drowsy for several hours, you cannot safely drive a car for the remainder of the day. Therefore, if this test is being done on an outpatient basis, a family member or friend must accompany you to the office in order to drive you home. If possible, you should choose someone with whom the doctor can freely discuss the results of your test. We request that your companion remain in the office during the test. You should arrive several minutes before your appointment and plan to stay approximately two hours. If the test is being done on an inpatient basis, a driver will not be needed. After the test, you will simply return to your hospital room to sleep off the remainder of the medication. You will be asked to remain in bed several hours to allow the sedation to wear off completely.
- Your Permission If you have any questions or concerns about this test, do not hesitate to ask your doctor about them. To signify that you completely understand what this test involves, you will be asked to sign a written consent form, or "permit," before the test begins.
Looking Inside
Prior to the test, you will be asked to remove your clothing and to slip into a patient gown. After signing the permission form, you will be positioned comfortably on your left side on the padded colonoscopy table. A small painless oximeter probe will be placed on your fingertip to monitor your pulse rate and breathing function during the exam. A thin nasal oxygen tube may be used to administer low flow oxygen during the exam. Then you will be given an intravenous injection of Demerol (pain killer) and Versed (tranquilizer); these medications will make you drowsy and relaxed, thus minimizing any discomfort during the examination. Please inform the doctor if you are allergic to Demerol or Versed, or if you chronically take narcotic painkillers such as Percodan, Percocet or Codeine, so that other medications can be substituted. Furthermore, rest assured that these medications will not prompt you to act or speak foolishly during the test.
..Your doctor will then examine and lubricate the rectal opening to allow simple passage of the colonoscope. This will not be painful, but is mildly uncomfortable for a few seconds. After the colonoscope is properly positioned, your doctor gently guides the scope through the colon, a process that takes approximately one-half hour. To improve visualization, your doctor gently infuses air into the colon. This may cause a sensation of abdominal fullness, but should not be painful. In fact, many patients actually fall asleep during the examination. As the test progresses, you may be asked to change your position now and then to facilitate the passage of the colonoscope through the colon.
Here is an xray of the abdomen taken during a colonscopy which demonstrates how far the scope travels into the colon all the way to the right side of the colon.
..Occasionally, passage of the colonoscope through the entire colon is impossible. While this may be caused by a blockage, it is most often caused by an extra "loop" of colon, adhesions from previous abdominal surgery, or severe diverticulosis. In such cases, a limited examination may be sufficient if the area of suspected abnormality has been visualized. If not, a barium enema x-ray (lower GI) may also be necessary.
..Taking SpecimensIf colonoscopy reveals any unusual condition such as inflammation, an ulcer, a tumor, or a polyp, your doctor may photograph it. This photo provides a permanent record for your medical chart and allows your other doctors to see what is wrong. With the advent of video-colonoscopy, it is now also possible to record the examination on a videocassette for later review when necessary. To better evaluate any areas of suspected abnormality, your doctor may take a brushing or biopsy of the colon lining. A brushing involves the passage of a tiny nylon brush through the center of the colonoscope. The brush rubs against the lining of the colon and retrieves bits of tissue for later analysis. To take a biopsy, the doctor passes a metal forceps through the scope and snips off a tiny sample of colon tissue for laboratory analysis. Both procedures are totally painless for the patient. Be assured that the decision to take a biopsy does not necessarily mean that your doctor suspects cancer. Biopsies of the digestive tract are often taken to look for other problems such as inflammation and ulcers.
..Removing Colon PolypsThe lining of the colon and rectum is normally smooth. Sometimes, however, growths known as "colon polyps" appear on the lining of the large intestine. Varying in size from pinheads to growths several inches in diameter, polyps do not usually produce any symptoms. Contrary to popular belief, polyps affect both men and women equally. Most colon polyps are initially non-cancerous. Nevertheless, as colon polyps continue to grow, they often develop into cancer of the colon. Colon cancer has become quite common in our society. In fact, nearly 1 in every 20 adult Americans will develop colon cancer in their lifetime. Colon cancer is now the leading cause of cancer deaths in nonsmokers. Only lung cancer takes a greater toll. It is not widely known that colon cancer now kills more women than breast cancer and more men than prostate cancer. But, there is good news. Research has confirmed that the single best prevention for colon cancer is the early detection and removal of all colon polyps!!! In the past, colon polyps located beyond the range of the proctoscope could only be removed by a major abdominal operation. Of course, this procedure required about a week of hospitalization and over a month of time lost from work for recovery. Fortunately, medical technology now permits the simple removal of most colon polyps. Should a small polyp be discovered during your colonoscopy, the polyp can usually be removed immediately. This prevents a potential colon cancer while eliminating the need for major surgery.
..
The doctor removes the polyp quite simply by placing a wire loop, or "snare," around the polyp's base and slowly tightening the loop. As the polyp is severed, a mild electric current cauterizes the tissue to prevent bleeding. There is no pain or any sensation as the polyp is removed. Polyp removal can usually be done on an outpatient basis. Moreover, since there is no incision, you may usually resume normal activity the next day.
..After The TestAfter an outpatient colonoscopy, you will be asked to rest awhile in the recovery room. Your companion will be asked to sit with you while the effects of the sedative begin to wear off. Once you are more alert, the doctor will meet with you to discuss the findings and any needed treatment. You will then be able to return home with your companion's assistance. However, since you will still be somewhat drowsy and uncoordinated, you will be taken directly to your car in a wheelchair by the office personnel. It is important that you go directly home; do not stop to eat along the way. Although you may resume a regular diet at home, you should eat lightly at first, and then gradually increase your intake of foods as tolerated. Since air was placed in the colon during the examination, you may experience the discomfort of mild "gas pains" for several hours until the gas is expelled. Because of the sedation's lingering effects, you should not drive, operate any machinery, drink alcohol, or engage in any vigorous activity for the remainder of the day. If the test is performed on an inpatient basis, you will be taken back to your hospital bed for recovery. If any specimens or polyps were extracted during the examination, the doctor will contact both you and your personal physician when the laboratory results become available. Further treatment or tests, if necessary, will be discussed at that time.
..Is This Test Dangerous?While every medical procedure involves some degree of risk, complications rarely occur in patients undergoing colonoscopy. With the advent of flexible fiberoptic instruments, this test has become a safe and simple method of directly examining the lower digestive tract. When performed by a physician who is specially trained and experienced in the procedure, the benefits of colonoscopy far exceed the risks.
..Your doctor is a Gastroenterologist. In addition to standard medical training, he has received special instruction in diseases of the digestive system and has been thoroughly trained in the safe and proper operation of the colonoscope. The combination of his expertise and your cooperation should make this test as safe and simple as possible. However, as with all medical procedures, complications can occur.
..The principal risks are perforation of the colon (a tear through the bowel wall) or bleeding. Although perforation generally requires surgery, certain cases may be treated with antibiotics and intravenous fluids. Bleeding may occur at the site of either a biopsy or polyp removal. Typically minor in degree, such bleeding may stop on its own or be controlled by cauterization. Occasionally, surgery is necessary. Fortunately, both perforation of the colon and bleeding are quite rare. Because bleeding may sometimes occur up to three weeks after a colon polyp has been removed, you should not plan to travel to any remote areas without medical access during this period of healing.
..Other possible risks include drug reactions and complications related to other diseases that you may have. Consequently, you should inform your doctor of all allergic tendencies and medical problems. Occasionally, the site of the sedative injection may become inflamed and tender for a short time. This is not serious. If inflammation occurs, applying warm compresses to the area is usually helpful. While any of these complications may occur, it is well to remember that each of them occurs quite infrequently. Your doctor will be happy to discuss the above risks with you further, especially with regard to your particular situation and need for colonoscopy.
..How About AIDS?Due to the recent extensive coverage of AIDS by the media, some patients have expressed the concern that they might, in fact, contract AIDS through this examination. Be assured that this is not the case. All our instruments are thoroughly cleaned and undergo high-level disinfection after each use. Only techniques known to kill all disease-causing bacteria and viruses, including the hepatitis and AIDS virus, are employed in this process.
..A Valuable Tool....In summary, colonoscopy is a valuable tool for the diagnosis and treatment of many diseases of the large intestine. Even when x-rays are normal, the cause of symptoms such as rectal bleeding or change in bowel habits may be determined by colonoscopy. It is also useful in the diagnosis and follow-up care of patients with colitis. Through colonoscopy, the detection and removal of colon polyps, and thus the prevention of colon cancer, are made possible. Periodic colonoscopy is a valuable tool in monitoring patients with previous polyps, colon cancer, or a family history of colon cancer. In essence, colonoscopy is a safe and worthwhile procedure that is extremely well tolerated. If you have any questions about your need for colonoscopy, do not hesitate to ask your doctor.